
A summary by Rev Rita Wong
Dr Chan Lai Gwen, together with translator Dr Lim Su Chi, gave us an understanding of mental health from a four-domain BPSS perspective. Thus mental unwellness would be – Biological (hardware – physical and neurological damage), Psychological (software – maladaptive emotional responses to life events), Social (environment – broken relationships and external stressors), and Spiritual (transcendence – the struggle and lack of faith).
Beginning with the Genesis account of creation, Dr Chan pointed out how guilt and shame (because of sin) led to fear and anxiety, which in turn led to hiding. Since then, anxiety has resulted in humans using all kinds of fig leaves to hide/cover their struggle.
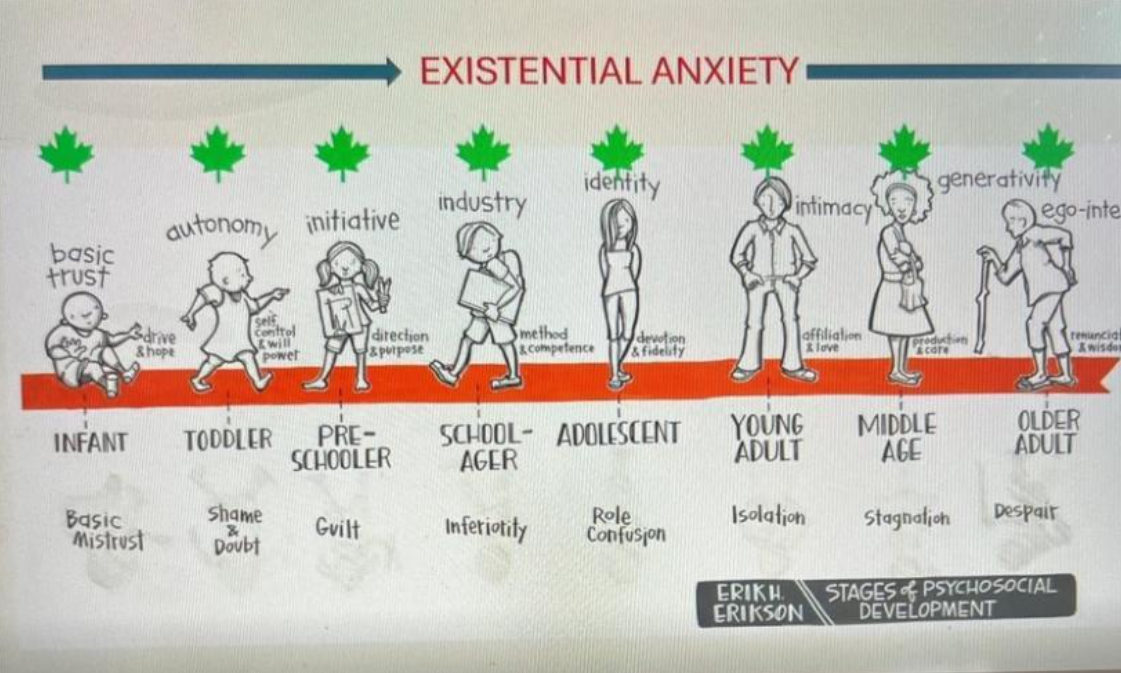
Erik H. Erikson’s life stages compare the healthy vs the maladaptive milestones of development.
The hippocampus is the seat of memory; the amygdala drives responses to stressors (fear, anxiety), and the prefrontal cortex is where judgment, wisdom and decision-making take place. The prefrontal cortex controls both the hippocampus and the amygdala.
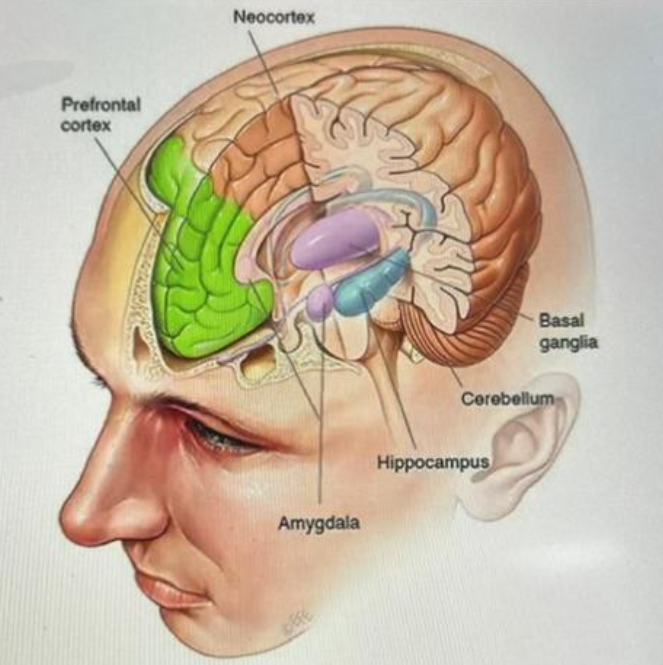
Hence, damage/less-ideal development of any of these parts of the brain results in how an individual responds to external triggers, even from a very young age. The example of a child being brought up in an orphanage by different adults leads to the child not knowing who to trust, thus seeing the environment/world as unsafe.
Psychosocial development goes on as brain development takes place. Earlier mal-development gives rise to negative responses, which produces problems in later development. Thus things we do to cover up fear/anxiety may not be perfect, even though the result may be good.
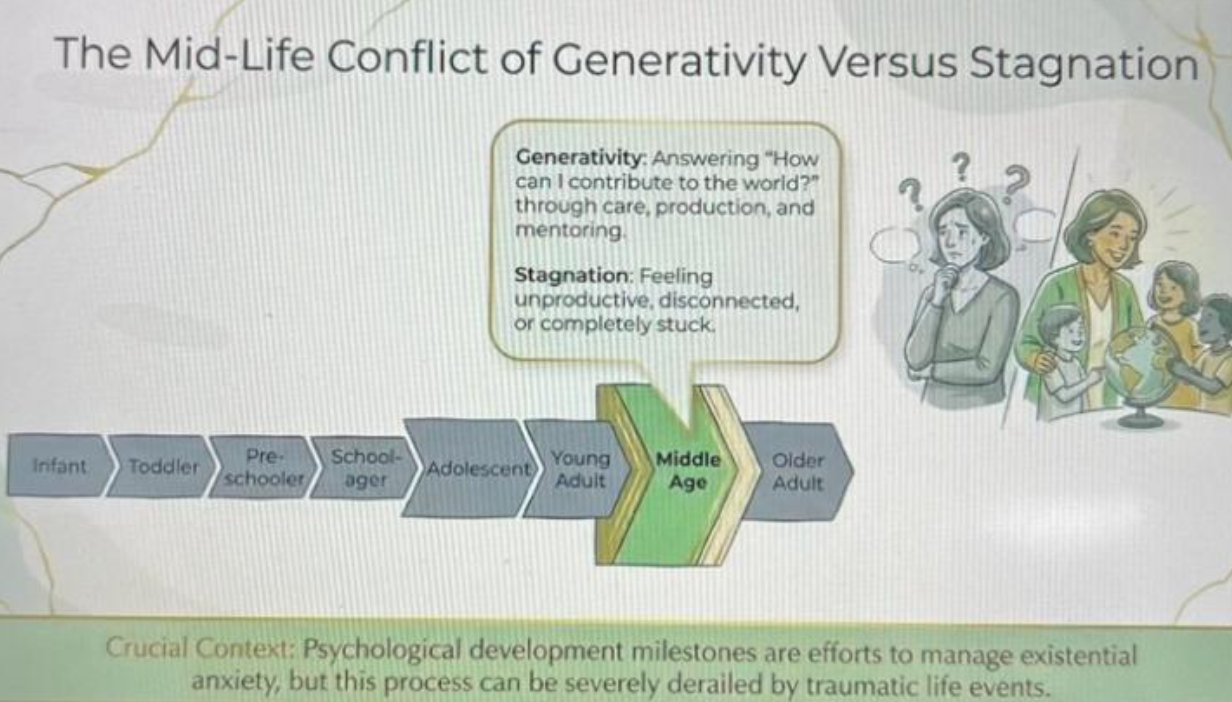
The core conflict in mid-life is the search for contribution and control vs the feeling of stagnation. Women tend to pour all their energy into their relationships (with family members as well as others) while men are more geared towards performance of self-sufficiency. Impending death, whether physical or of achievement/identity, produces anxiety and the resulting need to retain control.
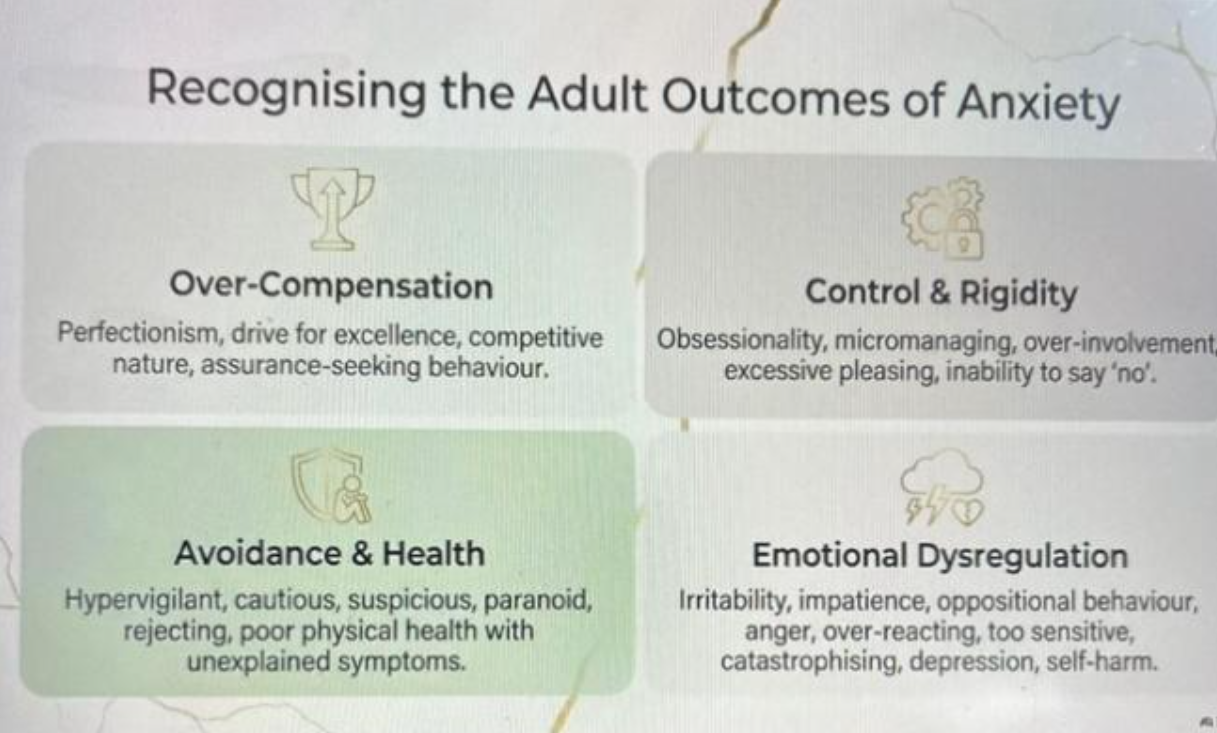
It is crucial to recognise adult outcomes of anxiety and to seek appropriate help.
There are various kinds of anxiety disorders, like OCD (Obsessive Compulsive Disorder), schizophrenia, bipolar disorder. Some are medical conditions and require treatment.
In the case of a suicidal person, symptoms are feeling trapped and hopeless, gradual disconnection with people, making wills and giving instructions for “When I am no longer around”. Two final tipping points are severe anxiety and restlessness (leading to acting without thinking), and wanting to connect with something (death) when connection with the world and people is felt to be completely lost.
Do not give up on a suicidal person. Speak openly because the person is still ambivalent about suicide. Establish a connection so that the person feels less alone and helpless. Connect the person to professional help.
The role of the church community is to give pastoral care and restore connection with God, to help the person to find hope.
In conclusion, it is important to be self-aware, and the four domains of BPSS guide us in our self-understanding. Where necessary, medication helps with the hardware, counselling helps the software, a supportive community anchors the social aspect, and spiritual resources aid in the connection with God. In seeking mental wellness, we seek the abundant life that God promises in John 10:10b (The Message) – “I came so they can have real and eternal life, more and better life than they ever dreamed of.”
Dr. Chan Lai Gwen is the Senior Consultant Psychiatrist at Tan Tock Seng Hospital. She specializes in the neuropsychiatry of stroke, traumatic brain injury, and Parkinson’s Disease. She is also the Adjunct Professor at Lee Kong Chian School of Medicine at NTU. In addition, she holds a Certificate in Faith Foundations from the Asia Pastoral Institute. She is very active in community service.
Dr. Lim Su Chi is the Co-Director of LKCMedicine’s Nutrition, Metabolism & Health research programme, Clinical Director of the Clinical Research Unit at Khoo Teck Puat Hospital, and Clinical Director of the Clinician Scientist Development Office at the National Healthcare Group (NHG) Group Research.
中年发展中的心理健康:从信仰视角出发
黄美兰牧师撰写的摘要
陈丽君医生与译者林舒奇医生共同从BPSS四维度的视角,帮助我们理解心理健康。因此,心理不健康可归因于:生物层面(硬件——身体和神经系统的损伤)、心理层面(软件——对生活事件的不适应性情绪反应)、社会层面(环境——人际关系破裂和外部压力源),以及灵性层面(超越性——信仰的挣扎与缺失)。
陈丽君医生从《创世记》的创世记述入手,指出内疚与羞耻(源于罪)如何导致恐惧与焦虑,进而引发逃避。自那时起,焦虑便促使人类使用各种各样的无花果叶来隐藏或掩盖自身的挣扎。
埃里克·H·埃里克森的人生发展阶段理论,对比了发展过程中的健康与不适应性里程碑。
海马体是记忆的中枢;杏仁核驱动对压力源(恐惧、焦虑)的反应;而前额叶皮层则是判断、智慧和决策发生的地方。前额叶皮层同时控制着海马体和杏仁核。
因此,大脑中任何这些区域的受损或发育不理想,都会影响个体对外部刺激的反应方式,即使是在非常年幼的时候也是如此。例如,一个在孤儿院由不同成年人抚养长大的孩子,往往会不知该信任谁,从而将环境或世界视为不安全的。
心理社会发展与大脑发育同步进行。早期发育异常会引发负面反应,进而导致后期发展出现问题。因此,尽管结果可能不错,但我们为掩饰恐惧或焦虑所采取的措施未必是完美的。
中年时期的核心矛盾在于:寻求贡献与掌控感,与停滞不前的感受之间的冲突。女性往往将全部精力投入到人际关系中(包括与家人以及他人的关系),而男性则更倾向于展现自给自足的能力。死亡的临近——无论是身体上的死亡,还是成就或身份的消亡——都会引发焦虑,并由此产生保持掌控感的需要。
认识到焦虑对成年人的影响并寻求适当的帮助至关重要。
焦虑障碍有多种类型,例如强迫症(OCD)、精神分裂症、双相情感障碍。其中一些属于医学疾病,需要接受治疗。
对于有自杀倾向的人来说,其症状包括感到被困住和绝望、逐渐与他人疏远、立遗嘱以及为“当我不在人世时”制定安排。最后两个临界点是严重的焦虑和躁动不安(导致不假思索地采取行动),以及在感到与世界和他人完全失去联系时,渴望与某种事物(死亡)建立联系。
不要放弃有自杀倾向的人。要坦诚地与对方交谈,因为对方对自杀仍持矛盾心理。建立联系,让对方感到不那么孤独和无助。帮助对方寻求专业帮助。
教会社区的角色在于提供牧养关怀,重建与上帝的联结,帮助当事人重拾希望。
总而言之,自我觉察至关重要,而BPSS的四个领域为我们的自我认知提供了指引。在必要时,药物治疗有助于改善“硬件”,心理咨询有助于调整“软件”,支持性的社区为“社会层面”提供支撑,而属灵资源则有助于与上帝建立联结。在追求心理健康的过程中,我们寻求的是上帝在《约翰福音》10:10b(《信息版圣经》)中所应许的丰盛生命——“我来了,是要叫他们得着真实且永恒的生命,比他们曾梦想过的更丰盛、更美好的生命。”
陈丽君医生是陈笃生医院的精神科高级顾问医生。她专攻中风、创伤性脑损伤和帕金森病的神经精神病学领域。她同时担任南洋理工大学李光前医学院的兼职教授。此外,她还持有亚洲牧养学院颁发的“信仰根基”证书。她非常积极地参与社区服务。
林舒奇医生是李光前医学院营养、代谢与健康研究项目的联合主任,邱德拔医院临床研究部的临床主任。